NAD+: Published Research
An evidence map of the NAD+ literature organized by what each study could actually measure: the biochemistry that defined NAD+ as a signaling substrate, the divergence between NR and NMN precursor pharmacokinetics, blood-based versus tissue-biopsy human trials, and the positive-versus-null result split that now shapes trial design. Educational reference.
For research use only. Not for human consumption. This article is educational reference material. It is not medical advice and is not a recommendation to use any substance.
How the NAD+ Literature Is Structured
Nicotinamide adenine dinucleotide (NAD+) occupies an unusual position in the research literature because it is simultaneously a classical redox cofactor and a consumable signaling substrate. That dual identity has produced two largely separate research streams that a reader can easily conflate. One stream, rooted in biochemistry and model organisms, asks how NAD+ is consumed by enzymes such as sirtuins and poly(ADP-ribose) polymerases (PARPs). The other, rooted in clinical pharmacology, asks whether supplying NAD+ biosynthetic precursors measurably raises the NAD+ pool in living humans and whether that shift tracks with any measurable physiological readout.
This article maps the literature along the axis that matters most for interpreting it: what each study was actually able to measure. Foundational biochemistry established mechanism in cells and yeast. Rodent studies established that the NAD+ pool is manipulable. Human trials, constrained by what can be sampled non-destructively, split further into blood-based and biopsy-based designs. Reading the evidence through that measurement lens explains why individual studies appear to disagree.
Findings from research models do not establish safety or efficacy in humans. Sparta Labs makes no claims about the use of this compound.
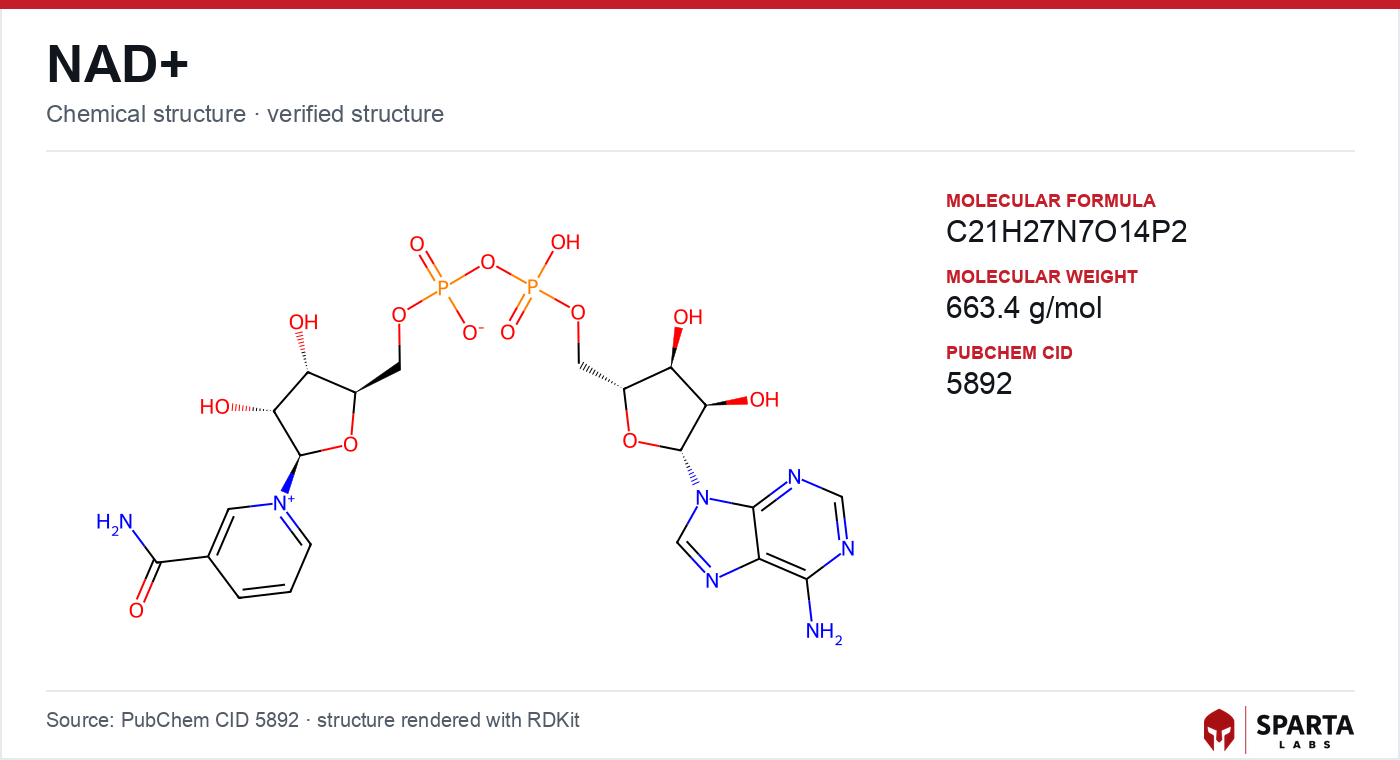
Figure: chemical structure of NAD+.
The Biochemistry That Reframed NAD+ as a Signal
For most of the twentieth century NAD+ was catalogued as a hydride carrier that shuttled between its oxidized (NAD+) and reduced (NADH) states in glycolysis and oxidative phosphorylation. The reinterpretation of NAD+ as a signaling molecule rests on a specific 2000 report. Imai, Armstrong, Kaeberlein, and Guarente demonstrated in Nature that Sir2, the founding sirtuin, is an NAD+-dependent histone deacetylase [1]. Working in Saccharomyces cerevisiae, the authors showed that Sir2 consumes NAD+ stoichiometrically for each deacetylation event, and that mutant enzymes retaining histone binding but lacking NAD-binding capacity lost catalytic activity. NAD+ dependency was therefore catalytically essential, not incidental.
The consequence of that finding is what organizes the downstream literature. If an enzyme consumes NAD+ as it works, then the size of the intracellular NAD+ pool becomes a rate-limiting variable, and different NAD+-consuming enzymes are placed in competition for a shared resource. Bai, Cantó, and colleagues examined exactly this in Cell Metabolism in 2011, reporting that genetic deletion of PARP1 in mice was associated with elevated tissue NAD+, increased SIRT1 deacetylase activity, and altered mitochondrial gene expression [2]. Pharmacological PARP inhibition produced comparable changes. The authors interpreted the results as evidence that PARP1 and SIRT1 draw on the same NAD+ pool, so the balance of consumption between them shapes downstream phenotype. This competition framework is described in more mechanistic detail in the NAD+ mechanism of action article.
Why Rodent Aging Studies Drove Interest in Precursors
A single rodent study did more than most to redirect attention toward supplying NAD+ precursors. Gomes, Price, Ling, and colleagues reported in Cell in 2013 that aged mouse tissues showed altered NAD+ concentrations relative to young controls, associated with reduced SIRT1 activity, normoxic nuclear accumulation of HIF-1 alpha, and a disrupted ratio of mitochondria-encoded to nuclear-encoded oxidative phosphorylation subunits [3]. The authors labeled this a "pseudohypoxic" state. Administering the precursor nicotinamide mononucleotide (NMN) to aged mice was associated with partial normalization of the mitochondrial gene-expression signature. That reversal, in a model organism, is the observation that seeded much of the subsequent translational program.
Parallel work characterized how a different precursor behaved. Cantó and colleagues reported in Cell Metabolism in 2012 that dietary nicotinamide riboside (NR) in mice produced dose-dependent elevation of hepatic and muscle NAD+, activation of SIRT1 and SIRT3 as read out by substrate deacetylation, and altered mitochondrial acetylation [4]. SIRT1-deficient mice did not reproduce the same responses, which the authors used to argue that NR's observed effects in that model were SIRT1-mediated. Both studies were preclinical, and neither addressed human translation. NAD+ biology also intersects with the mitochondrial-derived peptide literature; the signaling context of mitochondrial genome-encoded peptides is summarized in the MOTS-c mechanism of action article.
NR vs NMN: Two Precursors, Two Pharmacokinetic Stories
A recurring source of confusion is the assumption that all NAD+ precursors are interchangeable. The human pharmacokinetic literature treats NR and NMN as distinct, studied in separate trials with separate endpoints.
The first human pharmacokinetic study of oral NR was reported by Trammell, Schmidt, Weidemann, and colleagues, with Brenner as senior author, in Nature Communications in 2016 [5]. Across a dose-escalation and a small cohort, the authors documented dose-dependent increases in whole-blood NAD+ after oral NR. The study also identified nicotinic acid adenine dinucleotide (NAAD), not previously regarded as an intermediate in NR-to-NAD+ conversion, as a sensitive marker of NAD+ repletion. That biomarker discovery is analytically important because it gave later trials a validated readout beyond total NAD+.
NMN, by contrast, is anchored in the Science trial by Yoshino and colleagues at Washington University in St. Louis, published in 2021, enrolling 25 overweight or obese postmenopausal women with prediabetes [6]. Hyperinsulinemic-euglycemic clamp assessment reported greater insulin-stimulated skeletal muscle glucose disposal following NMN than placebo, and muscle-biopsy RNA sequencing identified NMN-associated changes in remodeling-related genes. The authors explicitly cautioned that findings from this specific population should be evaluated alongside other demographic groups before generalizing.
The Measurement Ceiling: Blood-Based vs Biopsy-Based Human Trials
The sharpest methodological divide in the human literature is not the precursor used but the tissue sampled. Because direct organ-level NAD+ measurement requires biopsy, most trials rely on whole-blood or peripheral blood mononuclear cell NAD+ as a surrogate.
Martens, Denman, Mazzo, and colleagues published a randomized, double-blind, placebo-controlled crossover trial of NR in Nature Communications in 2018, enrolling 24 healthy adults aged 55 to 79 [7]. Whole-blood NAD+ was reported to increase by roughly 60% during the NR period relative to baseline. The authors also reported reductions in systolic blood pressure and certain aortic-stiffness measures in participants with elevated baseline systolic pressure, while stating the trial was not designed to establish a causal link and framing these as observations warranting larger, purpose-built trials. This is a blood-based design: it established repletion in circulation but could not confirm target-tissue delivery.
Elhassan, Philp, Lavery, and colleagues crossed that measurement ceiling in Cell Reports in 2019, reporting a placebo-controlled crossover trial in 12 aged men who received NR, with skeletal muscle biopsies analyzed by targeted metabolomics [8]. The biopsies confirmed that NR elevated the muscle NAD+ metabolome directly, evidenced by accumulation of downstream metabolites, an advance over blood-only studies. RNA sequencing identified transcriptomic changes in energy-metabolism pathways. Notably, mitochondrial respiratory capacity measured by high-resolution respirometry did not differ significantly between NR and placebo, and the authors flagged the divergence between transcriptomic and functional readouts as an open question. That divergence, between a molecule reaching its tissue and a downstream functional endpoint moving, is one of the field's honest unresolved tensions.
The Positive-vs-Null Split and What It Tells Study Designers
Not every rigorously conducted trial reports a positive metabolic signal, and the null results are as informative as the positive ones. Dollerup, Christensen, Svart, and colleagues reported in the American Journal of Clinical Nutrition in 2018 a randomized, placebo-controlled trial of NR over 12 weeks in 40 sedentary obese men, with insulin sensitivity by hyperinsulinemic-euglycemic clamp as the primary outcome [9]. The primary endpoint did not reach statistical significance between NR and placebo, and secondary measures including resting energy expenditure, lipolysis, lipid oxidation, and body composition also did not differ significantly. The authors noted no serious adverse events attributed to NR, adding to the compound's tolerability record, and discussed how population differences, sedentary obese men versus the prediabetic or rodent populations elsewhere, might be a relevant design variable.
Read together, the Yoshino positive signal and the Dollerup null result are not a contradiction to be resolved by picking a winner. They differ in precursor (NMN vs NR), population (prediabetic postmenopausal women vs sedentary obese men), and endpoint framing. That heterogeneity is precisely what a systematic review by Gaspar and colleagues in the American Journal of Physiology-Endocrinology and Metabolism in 2023 catalogued when it evaluated the clinical evidence base and identified larger, longer-duration, and more population-specific trials as the central research priority [10].
Reading This Literature Without Overreaching
Three interpretive cautions follow directly from the structure above. First, a blood-NAD+ increase is a pharmacokinetic fact, not a functional outcome; the biopsy studies exist specifically because circulation is not the target tissue. Second, precursor identity matters, so NR data and NMN data should not be pooled casually. Third, the mix of positive and null primary endpoints across well-conducted trials is the current state of the evidence, not a flaw in it. Sparta Labs supplies NAD+ as research-grade material with batch-specific certificate-of-analysis documentation for laboratory investigation only.
NAD+ metabolism also sits inside a broader cellular-redox and antioxidant research context. Related endogenous redox chemistry is summarized in the glutathione published research article, and the compound's classification and discovery arc are covered in the NAD+ research overview.
References
-
Imai S, Armstrong CM, Kaeberlein M, Guarente L. Transcriptional silencing and longevity protein Sir2 is an NAD-dependent histone deacetylase. Nature. 2000;403(6771):795–800. DOI: 10.1038/35001622. https://pubmed.ncbi.nlm.nih.gov/10693811/
-
Bai P, Cantó C, Oudart H, Brunyánszki A, Cen Y, Thomas C, et al. PARP-1 inhibition increases mitochondrial metabolism through SIRT1 activation. Cell Metab. 2011;13(4):461–468. DOI: 10.1016/j.cmet.2011.03.004. https://pubmed.ncbi.nlm.nih.gov/21459330/
-
Gomes AP, Price NL, Ling AJ, Moslehi JJ, Montgomery MK, Rajman L, et al. Declining NAD+ induces a pseudohypoxic state disrupting nuclear-mitochondrial communication during aging. Cell. 2013;155(7):1624–1638. DOI: 10.1016/j.cell.2013.11.037. https://pubmed.ncbi.nlm.nih.gov/24360282/
-
Cantó C, Houtkooper RH, Pirinen E, Youn DY, Oosterveer MH, Cen Y, et al. The NAD+ precursor nicotinamide riboside enhances oxidative metabolism and protects against high-fat diet-induced obesity. Cell Metab. 2012;15(6):838–847. DOI: 10.1016/j.cmet.2012.04.022. https://pubmed.ncbi.nlm.nih.gov/22682224/
-
Trammell SA, Schmidt MS, Weidemann BJ, Redpath P, Jaksch F, Dellinger RW, et al. Nicotinamide riboside is uniquely and orally bioavailable in mice and humans. Nat Commun. 2016;7:12948. DOI: 10.1038/ncomms12948. https://pubmed.ncbi.nlm.nih.gov/27721479/
-
Yoshino M, Yoshino J, Kayser BD, Patti GJ, Franczyk MP, Mills KF, et al. Nicotinamide mononucleotide increases muscle insulin sensitivity in prediabetic women. Science. 2021;372(6547):1224–1229. DOI: 10.1126/science.abe9985. https://pubmed.ncbi.nlm.nih.gov/33888596/
-
Martens CR, Denman BA, Mazzo MR, Armstrong ML, Reisdorph N, McQueen MB, et al. Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults. Nat Commun. 2018;9(1):1286. DOI: 10.1038/s41467-018-03421-7. https://pubmed.ncbi.nlm.nih.gov/29599478/
-
Elhassan YS, Kluckova K, Fletcher RS, Schmidt MS, Garten A, Doig CL, et al. Nicotinamide riboside augments the aged human skeletal muscle NAD+ metabolome and induces transcriptomic and anti-inflammatory signatures. Cell Rep. 2019;28(7):1717–1728.e6. DOI: 10.1016/j.celrep.2019.07.043. https://pubmed.ncbi.nlm.nih.gov/31412242/
-
Dollerup OL, Christensen B, Svart M, Schmidt MS, Sulek K, Ringgaard S, et al. A randomized placebo-controlled clinical trial of nicotinamide riboside in obese men: safety, insulin-sensitivity, and lipid-mobilizing effects. Am J Clin Nutr. 2018;108(2):343–353. DOI: 10.1093/ajcn/nqy132. https://pubmed.ncbi.nlm.nih.gov/29992272/
-
Gaspar LS, Álvaro AR, Moita J, Cavadas C. Evaluation of safety and effectiveness of NAD in different clinical conditions: a systematic review. Am J Physiol Endocrinol Metab. 2023;325(5):E451–E465. DOI: 10.1152/ajpendo.00242.2023. https://pubmed.ncbi.nlm.nih.gov/37729025/
Disclaimer. Statements in this article have not been evaluated by the Food and Drug Administration. This compound is not intended to diagnose, treat, cure, or prevent any disease. Sparta Labs sells research-use-only materials. Content is provided for educational and informational purposes only and does not constitute medical advice. Consult a qualified medical professional for any health concerns.
Frequently asked questions
Why do human NAD+ precursor trials measure blood NAD+ instead of tissue NAD+?
Direct measurement of NAD+ inside a target organ requires an invasive tissue biopsy, so most human trials of nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) have used whole-blood or peripheral blood mononuclear cell NAD+ as a surrogate endpoint. Elhassan et al. (2019) and Yoshino et al. (2021) were notable because they obtained skeletal muscle biopsies, allowing direct confirmation that oral precursors raised the muscle NAD+ metabolome rather than only circulating levels.
What is the difference between NR and NMN in the published research?
Nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) are both NAD+ precursors studied in separate human trials. Trammell et al. (2016) reported the first human pharmacokinetic characterization of oral NR in Nature Communications, while Yoshino et al. (2021) reported a randomized trial of NMN in Science. The two compounds have been evaluated in different populations and endpoints, and the literature does not treat findings for one as interchangeable with the other.
Why did the NAD+ study by Imai et al. (2000) matter so much?
Imai, Armstrong, Kaeberlein, and Guarente reported in Nature (2000) that the sirtuin Sir2 is an NAD+-dependent histone deacetylase, consuming NAD+ stoichiometrically with each deacetylation event. This established NAD+ as a metabolic signal linked to epigenetic regulation rather than only a redox cofactor, providing the conceptual framework that much subsequent NAD+ research was built upon.
Do all human NAD+ precursor trials report the same outcome?
No. The published human trials are heterogeneous: some, such as Yoshino et al. (2021), reported changes in a metabolic endpoint, while others, such as Dollerup et al. (2018) in obese men, reported that the primary insulin-sensitivity endpoint did not reach statistical significance. This positive-versus-null split, across differing populations and endpoints, is a central feature reviewers have used to argue for larger and more targeted trials.